
COVID-19: Vaccinating kids – the debate heats up


By Maryanne Demasi, PhD
5- to 11-year-olds
This week, the Australian Federal Health Minister announced a commitment to COVID-19 vaccines for kids aged 5 to 11 years pending TGA-approval, after Pfizer claimed, in a press release, that it had obtained “favourable” results.
Pfizer’s ongoing Phase 2/3 trial apparently showed the vaccine “was safe, well tolerated and showed robust neutralising antibody responses”. However, the results were not submitted to the drug regulator, nor were they published in a medical journal, so for now, we must take their word for it.
Pfizer registered the trial plan, showing that it tested a lower dose (10µg) as well as two higher doses (20µg and 30µg) in 5- to 11-year-olds. Whether the vaccine can provide protection against symptomatic disease or severe COVID-19 remains to be seen.
The manufacturer also claimed that the vaccine had a “favourable safety profile”, however, it is important to note that the trial has not enrolled enough children (2,268) to detect any rare but serious harms that might arise from the vaccine
Only health kids were recruited in the trial – children with known or suspected immunodeficiency, a history of autoimmune disease, any condition associated with prolonged bleeding, anyone receiving treatment with immunosuppressive therapy or corticosteroids were excluded from the trial.
Notably, these are the same cohort of children who have been prioritised for the vaccine.
Despite little to no data available for its safety and efficacy, the Israeli Ministry of Health gave the green light to start vaccinating high risk 5- to 11-year olds with the lower-dose (10µg) of the vaccine.
Pfizer senior vice-president Dr Bill Gruber said he felt “a great sense of urgency” in the process, and Pfizer’s CEO Albert Bourla said trial data would be submitted to the various international drug regulators for “immediate authorisation.”
The language of Pfizer executives, the frenzied press coverage, and the political will of Governments, is all designed to pressure drug agencies to fast-track authorisations.
Younger than 5 years old?
Pfizer announced that trial data involving children under 5 are expected later this year.
Last week, Cuba began vaccinating toddlers as young as 2, using its homegrown vaccine, the Soberana 02, from the Finlay Vaccine Institute administered at adult doses. To my knowledge, there has been no data from Phase III trials published in the peer-reviewed literature in children as young as 2 with this vaccine.
China’s drug agency has cleared three COVID-19 vaccines produced by Sinopharm and Sinovac and is vaccinating children aged 3 years and older, under emergency use authorisation.
12- to 15-year-olds
Most major western nations have authorised COVID-19 vaccines for those aged 12 years and older.
In Australia for example, children aged 12 to 15 years began receiving the mRNA vaccines last week. According to the NSW Premier, 20% of children in the state of NSW have already had their first jab.
They require a two-dose regimen, the same dose given to adults, which aligns with the US FDA and Health Canada advisories on vaccines for this age group. (See my previous analysis for 12-15yr olds)
This does not align with the UK’s more cautious approach. After significant political and media pressure, UK chief medical officers recommended a single dose of the Pfizer vaccine, because of concerns about rare side effects such as heart inflammation.
Brazil appears to be an outlier at the moment. It was reported that the Minister for Health called for the suspension of the COVID-19 immunisation of people aged 12 to 17 after the death of a 16-year old girl named Isabelli Borges Valentim, eight days after she received the Pfizer shot. Authorities are still investigating the incident but the drug regulator denies any link to the vaccine.
Myocarditis/Pericarditis
This issue has stirred up some heated debate.
Now that real world data is becoming widely available, myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the membrane surrounding the heart) are being reported as rare harms related to the Pfizer & Moderna mRNA vaccines.
Israel, because of its fast vaccine roll-out, was first to raise the alarm - 148 cases of myocarditis were reported within 30 days of immunisation, more commonly after the second jab. It prompted the Israeli Ministry of Health to launch an investigation into any possible link between these cases of myocarditis and vaccination.
Since then, other countries such as the UK, the US and Canada have corroborating data.
In June, the US FDA decided that the link between the mRNA vaccines and myocarditis, particularly in young males, was sufficiently clear that it revised its vaccine fact sheets to include a warning.
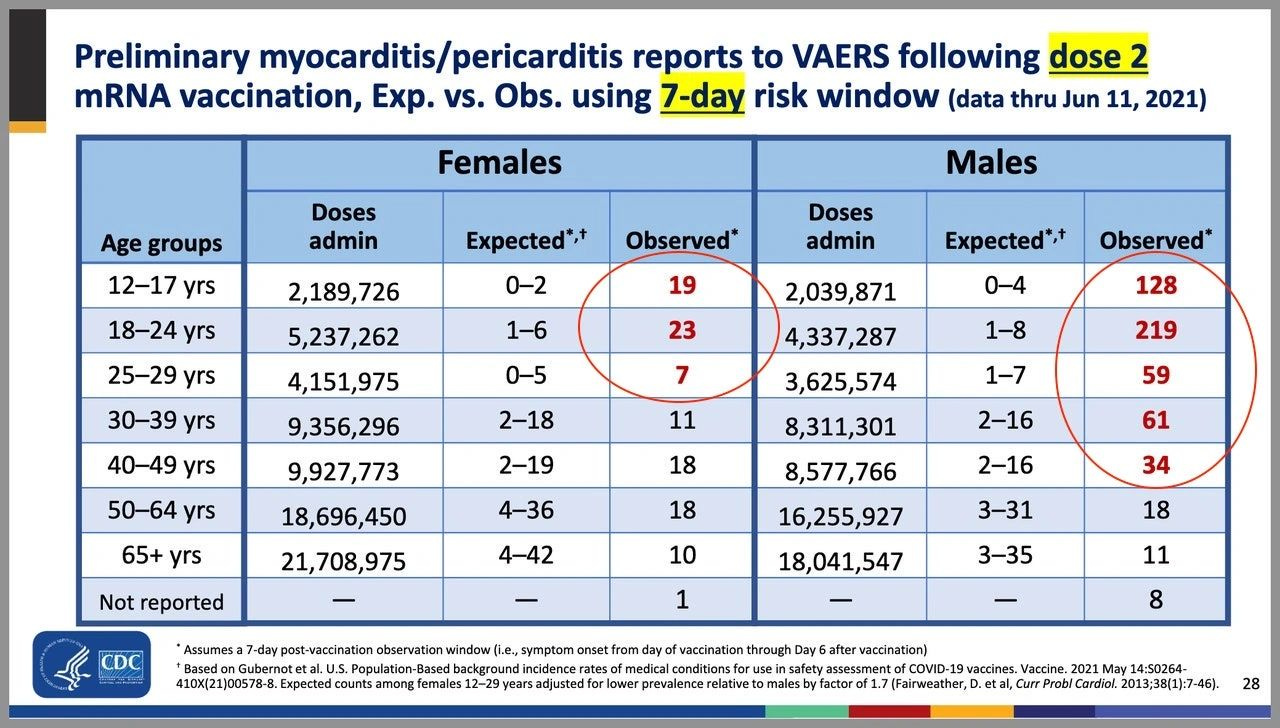
The CDC released data showing the incidence of “expected” versus “observed” incidences of myocarditis and pericarditis and found a significant increase in the observed rates. The graph shows the higher rates in red (see table numbers circled in red).
Another study, published in JAMA which looked at data from 40 hospitals in the US showed a similar pattern to the CDC, although at higher incidences, suggesting that the vaccine’s adverse events were being underreported.
Researchers then took a more granular look at the database for reported adverse events (VAERS database) between 1 January and 18 June, and found boys aged 12-15 years vaccinated with their second shot of the mRNA vaccine, with no underlying medical conditions were 4 to 6 times more likely to develop a cardiac adverse event, than ending up in hospital with COVID-19.
The study was published as a pre-print online but it ignited a twitter storm, with critics claiming the study ‘over-estimated’ the risk and it was biased because one of the authors belonged to a group that did not support making vaccines compulsory.
Sceptics say that most of the myocarditis cases are mild, and that children recover quickly from hospitalisation. Others are not so quick to dismiss the potential risk of ‘sub-clinical disease’ (myocarditis without symptoms) in children.
Notably, a retrospective multi-centre study across 16 US hospitals including patients <21 years of age with a diagnosis of myocarditis following COVID-19 vaccination, found concerning abnormalities in heart tissue (the left ventricle) (See image with yellow arrows).
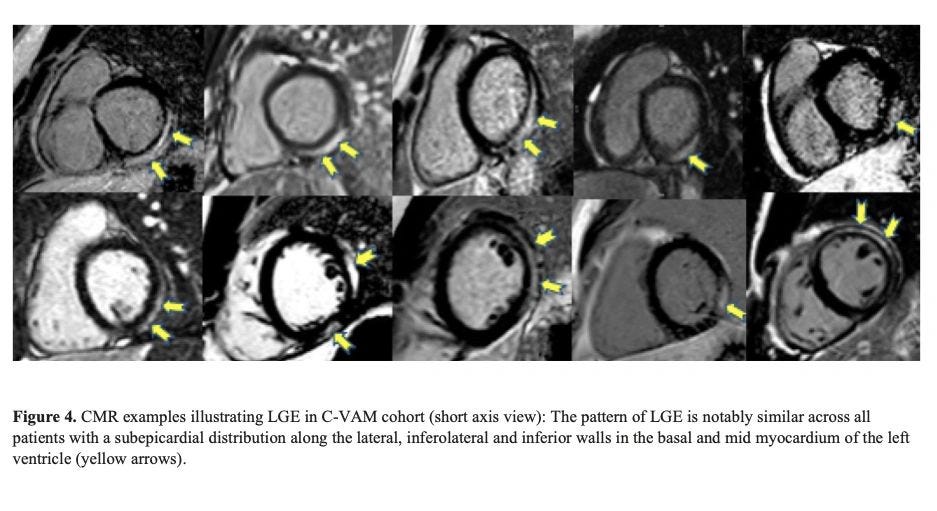
Careful monitoring is required to see if these abnormalities lead to fibrosis, which can have long-term implications for young patients.
Early findings suggest that post-vaccination myocarditis could be mediated by the toxicity of 'spike protein' on heart muscle cells or from circulating spike proteins in plasma after vaccination.
The risk of myocarditis associated with contracting COVID-19 infection may be higher than that after vaccination, but more research is needed to weigh harms against benefit.
If we don’t vaccinate kids, what about long COVID?
The fear of long-COVID has been a major impetus behind vaccinating kids.
A recent review by Monash University, analysing 14 international studies on long COVID in children and adolescents, found no difference in the symptoms reported by those who had experienced COVID-19 and those who had not.
Lead researcher on the study, Professor Nigel Curtis told newsGP the review’s findings should be reassuring for parents and carers.
Similarly, a webinar hosted by The BMJ revealed the results of the largest citizen-scientist participation study to date in young children. It used a smartphone app to monitor the illness and symptoms of children after testing positive to COVID-19.
The researchers found that the median duration of illness was 6 days. Only 4.4% of children had illness duration >28 days and 1.8% had symptoms >56 days. Encouragingly, their symptom ‘burden’ was greatly reduced by this time (none became worse) with the most common symptoms being headache and fatigue.
The researchers looked at neurological symptoms such as epileptic seizures, convulsions, impaired attention and concentration, but none were reported.
Lead investigator on the study, Prof Emma Duncan from Kings College in London concluded “Long illness duration of COVID-19 in children is uncommon.”
Vaccine Mandates for kids
Despite COVID-19 vaccine mandates for teachers in places such as New York and Australia (Victoria and New South Wales), no Federal government has announced plans to make the vaccines compulsory for children (yet).
Canadian and English professors have argued that making COVID-19 vaccines mandatory for children, will “encourage uptake”.
U.S. Surgeon General Vivek Murthy has also suggested that COVID-19 vaccine mandates for students could happen at the state and local level in the US, once they have been approved for paediatric use by the US FDA.
In a surprise announcement this week, the Los Angeles public school system said students aged 12 and older will now have to be double-vaccinated by the end of the year, to attend classes on campus or take part in sports and other extracurricular activities. It remains to be seen whether other school districts will follow.
Consent from kids
Before the age of 14, minors are generally thought to lack the cognitive capacity and maturity to make rational judgments about their health.
In fact, most US state laws presume that minors lack medical decision-making capacity and therefore require parental consent for most health care decisions, including vaccination, with some exceptions.
However, in the case of COVID-19, under what is termed 'Gillick competency', those under 16 years can make independent decisions about a medical treatment if they can demonstrate they have the capacity to consent, even if their parent withholds consent.

This applies to every Australian state and territory as part of the ‘common law’ and in the UK.
The Victorian government has produced ‘communication packs’ for teachers and educators on how to ‘promote’ COVID-19 vaccines to minors.
Hopefully, the conversations about COVID-19 vaccines, between health professionals and minors, are conducted without coercion, pressure or judgment.
Not surprisingly, this has raised the age-old question about who is better placed to determine the best medical treatment for a child – a parent or a Government minister?
The debate will continue and experts will need to wade through muddy waters to find a balance between protecting children’s health and the uncertainty over the long-term harms of the vaccine.