
Australian senate forces answers on why Covid vaccine deaths were not investigated
After US regulators linked child deaths to Covid-19 mRNA vaccines, an Australian senator has demanded to know why reported child deaths in Australia were not escalated for expert causality assessment.

GUEST POST
Dr Julie Sladden is a retired medical doctor in Australia committed to truth and transparency in healthcare.
When the US drug regulator announced it was investigating deaths linked to the Covid-19 vaccine, an Australian senator turned to our own regulator, the Therapeutic Goods Administration (TGA), to ask why the same scrutiny had never occurred here.
The answer, it turns out, is deeply unsettling.
Australia’s surveillance system had logged reports of deaths after Covid-19 vaccination — including deaths in children — yet almost none of those cases were referred for expert causality assessment.
Nearly three years would pass before Australia withdrew its recommendation to vaccinate healthy children.
Australia’s vaccine safety data
In September 2025, the National Centre for Immunisation Research and Surveillance (NCIRS) uploaded a report summarising Australia’s spontaneous surveillance data for adverse events following immunisation (AEFI) for Covid-19 vaccines administered in 2022.
Although dated March 2025, the report covers the second year of the Covid-19 vaccine rollout — including the first year the vaccines were offered to children aged 11 years and under.
The figures are stark.
In 2022, Australia recorded 18,398 adverse event reports following Covid-19 vaccination. Of these, 160 involved a fatal outcome. Six of the reported deaths occurred in children aged 0 to 17.
The report takes pains to clarify that “reporting a death to the TGA does not mean that the vaccine caused the death, or that the individual completing the report considers that the death was caused by a vaccine” and concludes that “safety monitoring continued to demonstrate a reassuring safety profile.”
However, the timing of these deaths complicates that claim.
Among children, the median interval between vaccination and death was 4.5 days. For young adults aged 18–29, it was just three days.
This is an important point. When an adverse event occurs shortly after exposure - within a timeframe consistent with known biological mechanisms - it strengthens the plausibility of a causal link and makes coincidence less likely. This principle underpins widely used causality frameworks such as the Bradford Hill criteria.
The overwhelming majority of the 160 reported deaths in the NCIRS Report occurred within a median of less than two weeks following vaccination. This fact casts doubt on the “reassuring safety profile” asserted by the report.
Surprisingly, the report states, “Only one death following a Covid-19 vaccine administered in 2022 was assessed by TGA as likely to be causally linked to vaccination.”
At first glance, that conclusion seems remarkable. It becomes less surprising once one learns that only two of the 160 reported deaths — and none of the six child deaths - were referred to the Vaccine Safety Investigation Group (VSIG) for expert causality assessment.
Senator Antic questions the TGA
Why, then, were none of the reported child deaths escalated for expert investigation?
The TGA was asked this exact question by Senator Alex Antic during the December 2025 round of Senate estimates.

Responding on behalf of the regulator, Dr Daniel Dascombe, acting principal medical adviser in the TGA’s pharmacovigilance branch, explained that the VSIG had been convened during the early phase of the rollout for specific conditions such as myocarditis and thrombosis with thrombocytopenia syndrome.
At that time, he said, the risk–benefit profile of Covid-19 vaccines was still being characterised, and the potential impact of serious adverse events on that balance was unknown.
“As time progressed,” he told Senator Antic, “the safety profile of these vaccines has become better established, and the grounds for establishing a VSIG to look into specific case reports have changed over time.”
However, that explanation did not address the question being asked by Senator Antic.
The deaths recorded in 2022 did not occur years down the track once safety was settled. They occurred during the early stages of rolling out a new vaccine program to children using a novel technology, at a time when “the potential impact of these adverse events on the risk–benefit balance… was unknown.”
Yet the VSIG was not convened in response to any of the reported child deaths, even though healthy children were known to be at minimal risk from Covid, and that death as an adverse event clearly “has the potential to change the favourable benefit–risk balance of the vaccine,” a stated criterion in the VSIG work instruction.
Notably, the VSIG can only be convened following agreement between the TGA and the Office of Health Protection and must adhere to clearly documented criteria and guidance outlined in the WHO’s Global Manual on Surveillance of Adverse Events Following Immunization.’
A possible explanation for why so few deaths were escalated for causality assessment lies in a recently released TGA document obtained under freedom-of-information (FOI) laws.
The document outlines a “pilot” AEMS Preliminary Fatal Case Assessment process, used by TGA staff to screen fatal cases before referral to the expert panel.
It instructs staff to avoid “burning out” the VSIG panel by not referring cases that do not meet defined criteria, or where essential documentation — such as finalised autopsy reports — is not yet available.
The document attributes this approach to guidance from the WHO.
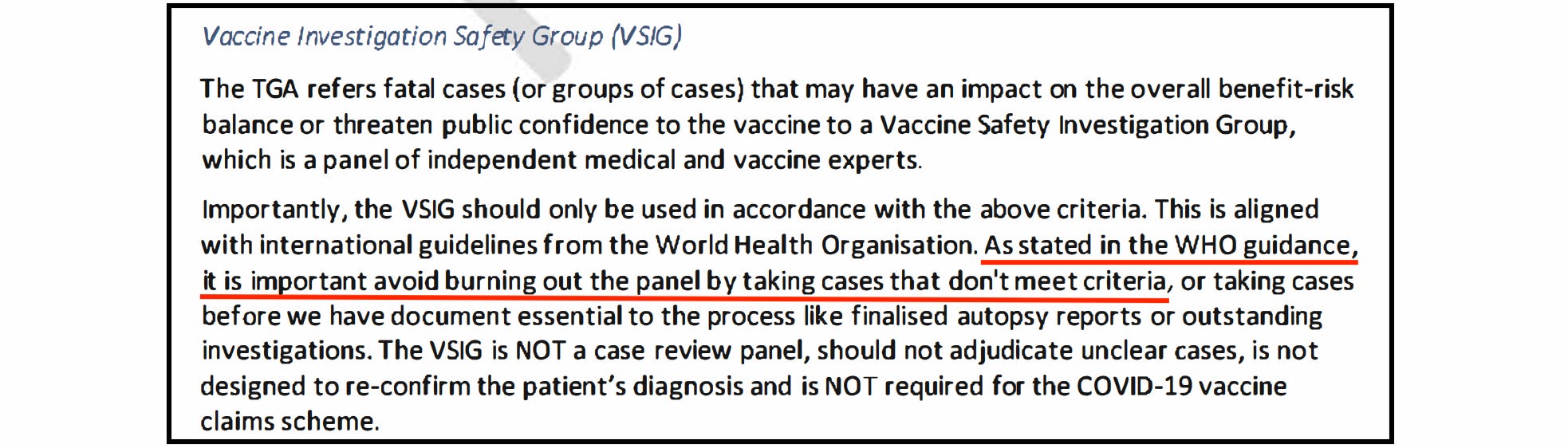
But that attribution is false — the WHO guidance contains no reference to avoiding panel “burn out,” nor does it advise restricting referrals for that reason.
On the contrary, the guidance stresses that causality assessment of serious adverse events requires specialist expertise and explicitly recommends that countries lacking sufficient in-house capacity should seek assistance from the respective WHO country or regional office.
Is this why only two of the 160 reported deaths, and none of the six reported deaths in children, were referred for expert causality assessment – to avoid “burning out” the panel?
A policy reversal, three years too late
On 27 March 2025 the recommendation for healthy children to receive Covid vaccines, was quietly withdrawn. There was no political announcement, no press conference and little media attention.
The change came via a brief statement by the Australian Technical Advisory Group on Immunisation (ATAGI) advising that recommendations for healthy children under 18 had been revised.
Two months later, the Australian Immunisation Handbook was updated to reflect that the “risk of severe illness is extremely low in this cohort over the course of the pandemic, and benefits of vaccination are not considered to outweigh the potential harms.”
This assessment was not new. The minimal risk posed to children from the disease had been known since 2020.
From the first reported child death to the policy reversal, it took nearly three years.
During that critical period, reports of death — an adverse event with the potential to overturn a favourable benefit-risk balance — were filtered out rather than escalated and investigated.
This was a failure of the process in real time.
The VSIG framework exists precisely for rare, serious, and uncertain safety signals - especially in low-risk populations. That it was not invoked in response to reported child deaths raises unavoidable questions about how safety thresholds were interpreted, how WHO guidance was applied, and whether institutional caution gave way to bureaucratic paralysis.
If vaccine safety surveillance is to restore public trust, these decisions and the internal instructions that shaped them, must now be examined with the same rigour that regulators so often claim, but have applied so selectively.
Acknowledgement: The author thanks Dr Melissa McCann for her input.