
Trapped in the Spider Web: How Big Pharma Captured Our Healthcare System
GUEST POST written by Kim Witczak


Kim Witczak is a drug safety advocate and the co-founder of Woody Matters, a non-profit organisation dedicated to pharmaceutical reform. She became an activist after the tragic death of her husband, Woody, who died by suicide in 2003 after being prescribed the antidepressant Zoloft. Since then, she has worked to raise awareness about the risks of psychiatric drugs and the shortcomings of regulatory agencies like the FDA, where she has also served as a consumer representative on advisory committees.

I never set out to be an advocate. I wasn’t a doctor, scientist, or policy expert. I was just a regular person who, like so many, blindly trusted that our healthcare system was designed to protect us.
But life has a way of pulling us into the arena when we least expect it.

The Story of the Accidental Advocate - KIM WITCZAK - Click to read full story
After the tragic and unexpected loss of my husband Woody to the antidepressant Zoloft that he was prescribed for insomnia, I was thrust into a world I never imagined—one where medicine wasn’t solely about healing, but deeply entangled in a system that prioritizes profit over safety, buries harms, and keeps the public in the dark.
For over two decades, I’ve had a front-row seat to how this system truly operates—not the illusion of rigorous oversight we see in medical journals or glossy pharmaceutical ads, but the reality of how industry influence is woven into every stage.
I’ve met with regulators, testified before the FDA and Congress, filed a wrongful death and failure-to-warn lawsuit against Pfizer, and earned a seat on the FDA’s Psychopharmacologic Drugs Advisory Committee as a consumer representative.
I’ve also spoken at, and participated in, global conferences like Selling Sickness, Too Much Medicine, and the Harms in Medicine meeting in Erice, Italy—where some of the world’s leading experts acknowledge what few in mainstream medicine dare to say:
Our healthcare system isn’t about health—it’s about business.
And in this business, harm isn’t an accident. It’s built into the system.
The more I uncovered, the more I realized:
We aren’t just patients. We are customers.
And we are all trapped in Big Pharma’s spider web of influence.
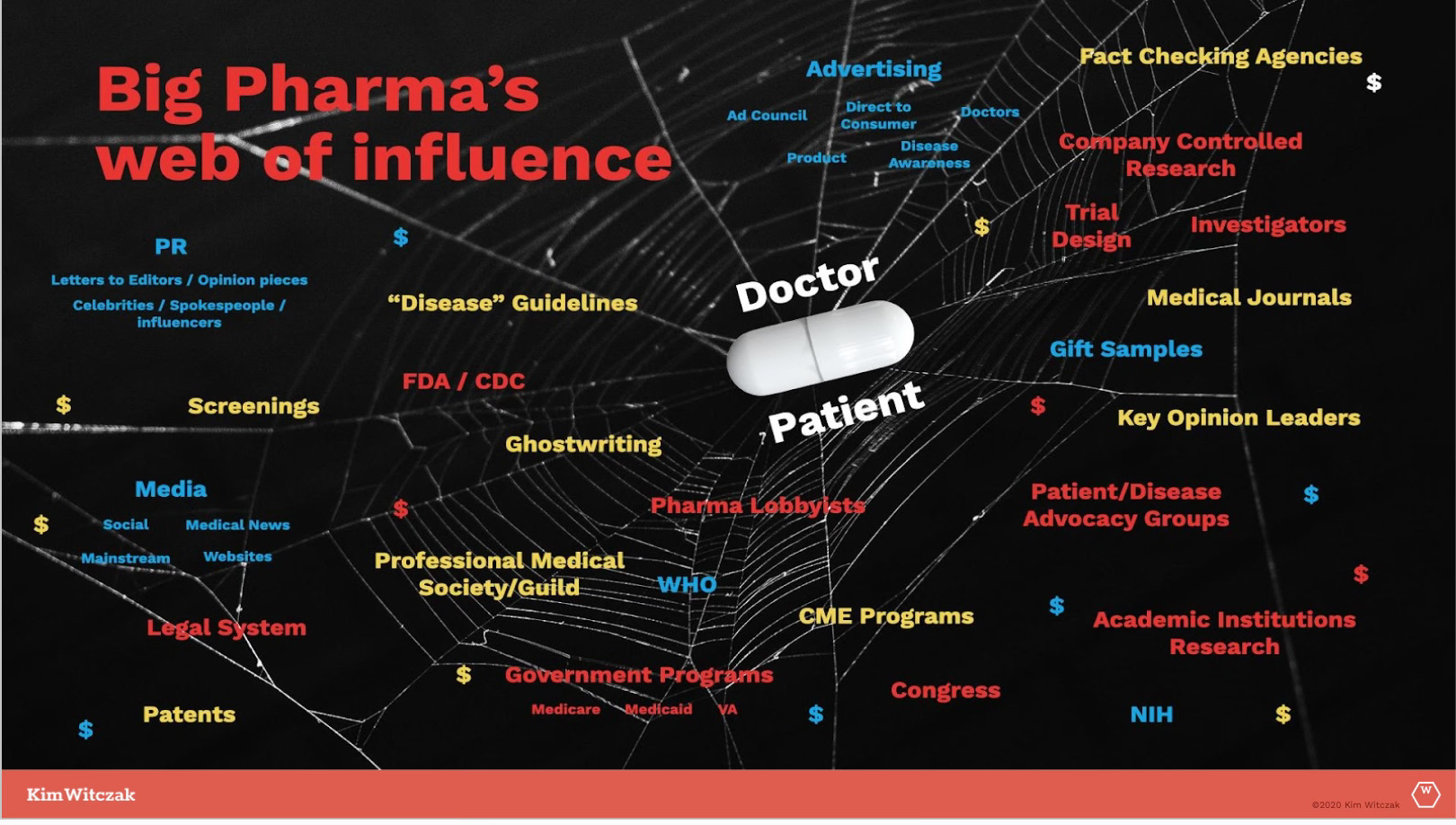
The Spider Web of Influence
The more I learned, the more I saw just how deeply embedded the pharmaceutical industry is—not just in drug development and marketing, but in every corner of our healthcare system.
That’s why I created the ‘Big Pharma Spider Web of Influence’—to visually map out how the system is designed not to prioritize health, but to sell sickness while minimizing, downplaying, or outright hiding harms.
From clinical trial design to regulatory approval, from direct-to-consumer advertising to medical education, from controlling medical journals to silencing dissenting voices, the industry has built an intricate and self-reinforcing web—one that traps doctors, patients, and even regulators in a cycle of pharmaceutical dependence.
How the Web Works
Clinical trials are often designed, funded, and controlled by the very companies that stand to profit. They manipulate data to exaggerate benefits and obscure risks, ensuring that negative results are buried, spun, or never published at all.
Regulatory agencies like the FDA are deeply entangled with the industry they’re supposed to oversee. More than 50% of the FDA’s budget comes from industry-paid user fees, and a revolving door ensures that many key decision-makers come from—and later return to—pharmaceutical companies.
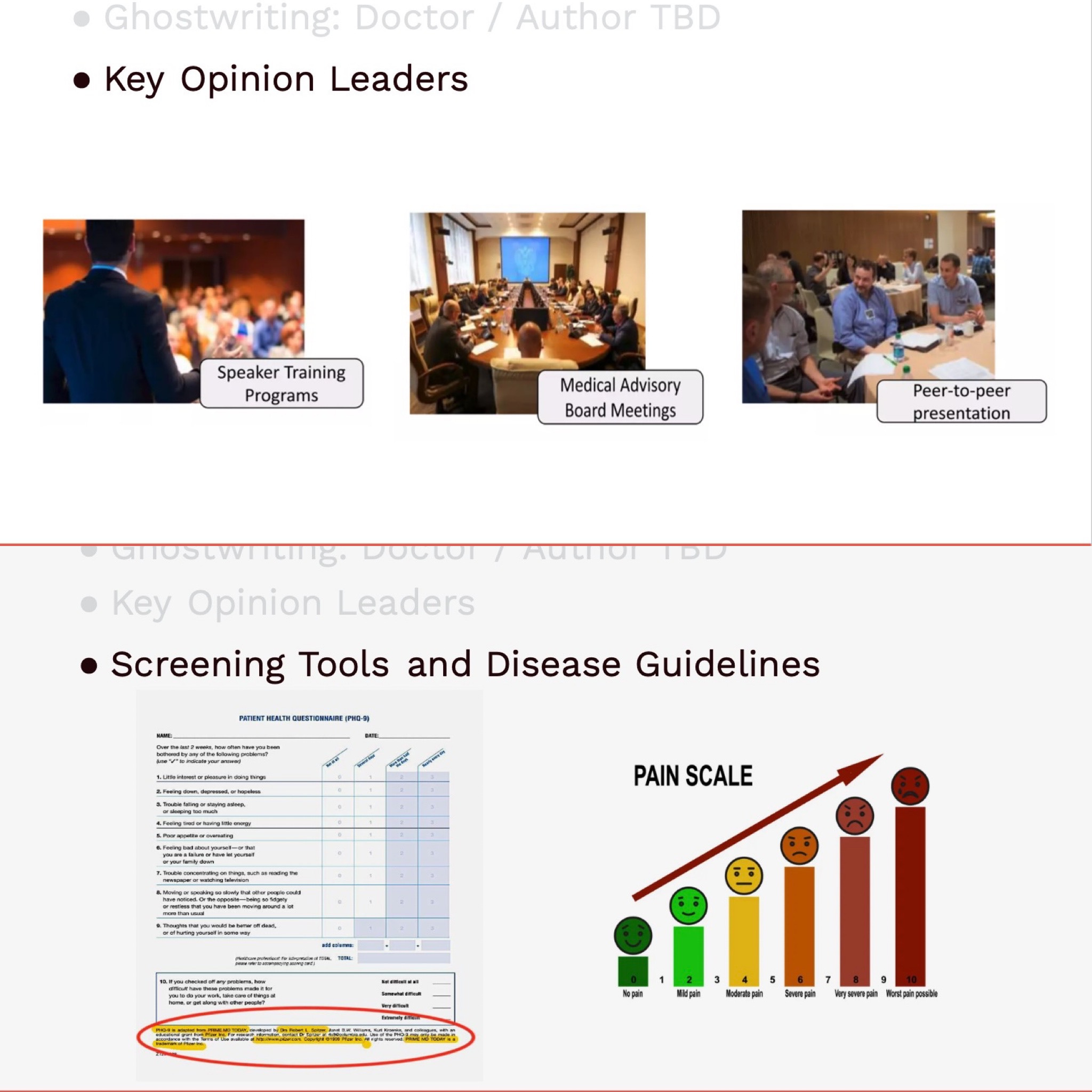
Medical journals depend on pharmaceutical funding through advertising, reprint sales, and industry-sponsored studies—severely limiting independent scrutiny of drug safety. Many studies are ghostwritten or crafted by paid “key opinion leaders” (KOLs) who serve as pharma’s trusted messengers.
Doctors receive education through industry-funded programs, learning “best practices” based on treatment guidelines crafted by the very system that profits from overprescription.
Patient advocacy groups, once independent grassroots organizations, have been co-opted by industry money, ensuring that the loudest voices often serve pharma’s interests rather than patients’ needs. I call them “astroturf” patient groups—they look like real grassroots organizations, but they’re anything but.
Screenings and guidelines continuously expand the definitions of disease, turning more people into lifelong customers.
This isn’t about one bad actor or isolated corruption—it’s a systemic issue. The entire structure is designed to push more drugs onto the market, medicalize normal human experiences, and only acknowledge harm when it becomes too big to ignore.
It’s a brilliant business model—but a catastrophic public health strategy.
“To Sell to Everyone”: The Business Model of Medicine
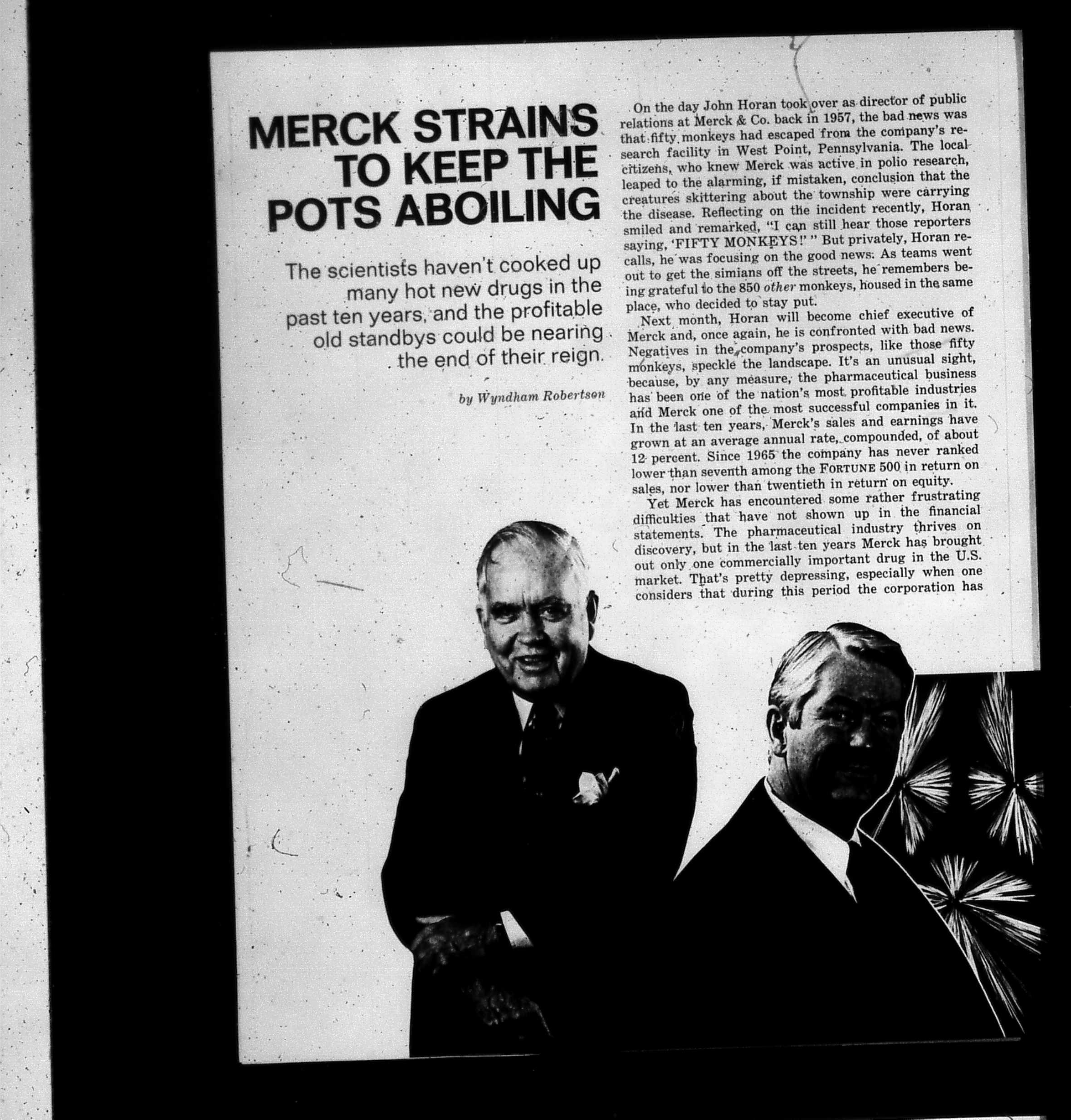
If this sounds like a conspiracy, consider the bold admission made by Henry Gadsden, former CEO of Merck, in a 1976 interview with Fortune Magazine:
“The problem we have had is limiting the potential of drugs to sick people. We could be more like Wrigley’s Gum… it has long been my dream to make drugs for healthy people. To sell to everyone.” - Former Merck CEO Henry Gadsden
Let that sink in.
This wasn’t about curing disease—it was about expanding markets. Gadsden’s vision wasn’t just to treat illness, but to medicalize everyday life—creating a cradle-to-grave model where every person, healthy or sick, became a customer for life. Just like selling a variety of gum—something for everyone. Juicy Fruit, Big Red, Doublemint, Spearmint, and so on.
And that’s exactly what happened.
Today, we live in a system where:
Everyday emotions—sadness, worry, shyness—are rebranded as medical conditions requiring treatment.
Preventive medicine often means lifelong prescriptions, not lifestyle changes.
Drugs are marketed to the “worried well”, turning normal human experiences into diagnoses.
This isn’t just theory—it’s well documented. In Selling Sickness: How the World’s Biggest Pharmaceutical Companies Are Turning Us All into Patients, Ray Moynihan and Alan Cassels expose how pharmaceutical companies create diseases, expand diagnostic criteria, and convince the public that normal life experiences require medical intervention.
The goal?
Make medication the default—not the last resort.
Harms Are Always an Afterthought
Harms from medication are not rare, nor are they unexpected.
But in this system, they are treated as acceptable collateral damage—something to be dealt with only after the damage is done, after lives are lost or forever changed.
I’ve sat in FDA Advisory Committee meetings, reviewing new drug applications, and have seen firsthand how safety concerns are often dismissed in favor of “innovation” or “unmet medical need.”
I’ve heard industry representatives and advisory committee members argue that safety signals can be addressed post-market, meaning after a drug is already in circulation and causing harm or a required REMS (Risk Evaluation and Mitigation Strategies) program upon approval.
But by the time post-market safety issues are acknowledged, it’s often too late.
We’ve seen this play out over and over:
Opioids—marketed as “non-addictive” and pushed aggressively onto patients, leading to an epidemic of addiction and death.
SSRIs and antidepressants—long linked to increased risks of suicide and violence, particularly in young people, yet downplayed or dismissed for decades. Other hidden harms include withdrawal syndromes and Post-SSRI Sexual Dysfunction (PSSD), conditions that many patients were never warned about.
Antipsychotics—widely prescribed for off-label use, leading to severe metabolic and neurological side effects.
COVID-19 vaccines—an experimental mRNA platform rushed to market, mandated, and imposed on society despite limited long-term safety data and growing concerns over harms.
Every time, the pattern is the same:
The industry sells the benefits while downplaying the risks—until those risks become too big to ignore.
By then, the drug is a blockbuster, billions have been made, and the system moves on to the next new “breakthrough.”
More Than Degrees: The Truth of Lived Experience
One of the biggest lessons I’ve learned in this fight is that real-world experience matters just as much as credentials.
Over the years, I’ve been invited to speak at medical schools, PhD programs, and universities, thanks to brave academics willing to challenge the narrative. I share my journey as an accidental advocate—someone who didn’t have a medical degree but discovered America’s broken drug system the hard way.
But let’s be honest—the medical world is driven by credentials. Or as I like to say, the alphabet soup.
At conferences, attendees wear name tags listing their titles—MD, PhD, JD, MPH. It’s a quick way to size someone up, to assess credibility before even speaking. And I’ve seen it happen: people glance at my name tag, see no impressive letters after my name, and walk right by.
Years ago, I was speaking at the Preventing Overdiagnosis Conference and noticed my badge read: Kim Witczak, BA.
I was horrified. Was that really necessary? Did my name tag need to remind everyone that I only had a BA?
Later, I was telling the story to a doctor friend, and he laughed.
“Next time, tell them BA stands for Bad Ass.”
And he was right.
Because real expertise doesn’t always come from an advanced degree—it comes from lived experience, from asking the right questions, from refusing to accept the status quo.
The Counterargument: But Don’t We Need Experts?
Of course, some will argue that only experts with MDs and PhDs should be trusted to shape healthcare policy.
But that assumes that the system they operate in is free from bias, conflicts of interest, or financial incentives.
The reality is, many of those with the most letters after their names are also the ones benefiting from pharma funding—whether through consulting fees, research grants, or advisory roles.
Meanwhile, patients and their families—the ones living with the consequences—are too often ignored.
That needs to change.
Asking Better Questions: Reclaiming Our Power
If there’s one thing I’ve learned on this journey, it’s this: no one is coming to save us. The institutions meant to protect us are too entangled in the web to act with true independence.
My late husband, Woody, used to say: “Follow the money.” And when you do, the truth becomes impossible to ignore. Pharmaceutical profits—not patient well-being—drive the system. That’s why the only way to create real change is through awareness, transparency, and fundamentally shifting how we think about medicine and health.
That starts with asking better questions:
Who funded this research?
Does this person or institution have financial ties, intellectual bias, or self-interest that could impact their recommendations?
Who benefits from this treatment?
What aren’t we being told?
What are the long-term consequences of this drug or intervention?
Are there safer, non-drug alternatives being ignored because they aren’t profitable?
But asking the right questions isn’t enough.
We have to stop outsourcing our health to a system built on financial incentives and guided by corporate interests.
We must demand full transparency, challenge the status quo, and recognize that sometimes the best medicine isn’t a pill, but a deeper understanding of what our bodies truly need.
Because once you see the web, you can’t unsee it.
And once you recognize how deeply medicine has been shaped by profit, you’ll realize the most important question isn’t just “What can I take?”—it’s “Who benefits if I do?”
Final Thoughts: Tearing Down the Web
I never wanted to be in this fight, but once you see the web, you can’t unsee it. That’s why I continue to speak out, to challenge the system, and to push for real accountability.
Because the stakes aren’t theoretical. They’re deeply personal.
For me, this fight began over two decades ago with Woody. But for countless others, it begins the moment they or someone they love is caught in the web—trusting a system that was never truly designed to protect them.
It’s time to tear down the web.
And it starts with seeing it for what it really is.
Inspirational. Thanks Maryanne
Just this week I saw a patient recovering from necrotising myositis after being prescribed statins for a minor elevation in LDL and no other risk factors.
She also now has cardiomyopathy from either/or statins and Civid jabs.
She will never recover.
I also saw a woman who has myopathy from statins.
Her husband, also on long term statins, has severe dementia, which she blames on the statins.
Her GP tells her she will have a stroke if she stops them.
She has mildly elevated LDL and no other cardiovascular risks.
She is fully aware of the problem and was very happy to cease them at my suggestion.
Doctors are willing pawns in the game.
A huge capacity to remember medical flowcharts but zero creative or critical thinking intelligence.